The Blue Cross Blue Shield of Massachusetts Foundation has a different format for its 2011 Annual Report - six health care experts ask and answer questions. The six are MA Governor Deval Patrick, recent CMS Chief Don Berwick, Neighborhood Health Plan chief Deb Enos, Boston Medical Center CEO Kate Walsh, Associated Industries of MA President Rick Lord, and me.
Here's the link.
Friday, March 30, 2012
Wednesday, March 28, 2012
The Supremes Strike a Blow for Health Care Affordability
Today’s Managing Health Care Costs Indicator is $3000
The Supreme Court last week ruled that Prometheus Pharmaceuticals could not patent a test that suggests medication dose changes based on amount of metabolites in the patient’s blood. Mayo Clinic had developed a similar test – with its own validated normal range, but Prometheus sued to stop Mayo from marketing its test. Now there can be competition in this field, which is likely to lead to more innovation and lower price.
This has led the Supreme Court to ask an appeals court to review its earlier finding that Myriad Pharmaceuticals and the University of Utah could continue to be the sole owners of a patent for BRCA 1 and 2 – the genes that are associated with heightened risk of breast and ovarian cancer, especially among Ashkenazi Jews. The genetic test for these genes now costs $3000 – and many insurers are reluctant to provide coverage.
Advocates periodically assert that “personalized medicine” can improve quality and outcomes while lowering overall resource costs, and point to tests that can protect patients from drugs that would offer them no benefits, and help determine the best dose based on genes rather than trial and error. There is no question that genetic testing is already saving and improving lives. The current high expense of genetic tests makes it unlikely we can achieve the goal of cost savings - and single source manufacturers would fight hard to maintain high “brand name” prices. These Supreme Court decisions can inject competition in the biotechnology market, offering the prospect of price relief in the all-important market of genetic tests and gene therapies.
Tuesday, March 27, 2012
The Perils of Low Cost Medicine
I’ve often posted about “accretive innovation,” new medical technologies that cost a lot, and offer only a small portion of patients what is often only a tiny benefit. I've talked less about the consequences of when prices are too low - which means we'll not obtain the potential societal benefits of a new drug.
First, an example of accretive innovation.
In 2001, Xigris (human activated protein C, Lilly) was approved for use in severe sepsis based on a small study. The drug was heavily marketed by Lilly – including hiring a PR firm and secretly funding an ethics task force which came up with guidelines that promoted Xigris use. Subsequent studies showed that the drug was associated with a higher risk of brain bleeding and did not improve survival rates. The drug was withdrawn from the market last fall. The result of all of this marketing is that a wildly expensive drug ($8000 per dose) gained high market acceptance; sales were $200 million per year.
I’m reminded of the Xigris story by the New York Times last week, which reported that tranxemic acid, a dirt-cheap generic medication, could save up to 128,000 lives a year, 4000 of them in the US.
From the Times report:
For months, a simple generic drug has been saving lives on America’s battlefields by slowing the bleeding of even gravely wounded soldiers.
Even better, it is cheap. But its very inexpensiveness has slowed its entry into American emergency rooms, where it might save the lives of bleeding victims of car crashes, shootings and stabbings — up to 4,000 Americans a year, according to a recent study.
Because there is so little profit in it, the companies that make it do not champion it.
This isn’t the first time we’re seeing the ugly side to drugs costing too little. We have serious shortages of generic oncology medications and generic attention deficit disorder medications right now. We need effective drug company marketing to bring pharmaceutical innovations to physicians – but disseminating knowledge about drugs is difficult if there is no one with a profit motive to do so.
I was aghast at the FDA approval of brand name colchicine, a drug that cost pennies, was well-accepted for gout and other indications, and which skyrocketed in price to over $5. I felt rage when the Wall Street Journal reported that a pharmaceutical would charge $1500 for a previously-generic $20 progesterone injection to prevent premature deliveries. But perhaps my anger is at least partially misdirected.
It’s obvious that we can’t afford ridiculously high prices for drugs. It's a bit less obvious but no less true that we need high enough prices for effective drugs that their makers will manufacture them and market them for appropriate use.
Monday, March 26, 2012
Doc Dude Gives in to High Tech Medicine
by: costguy
Be sure to read a blog about GE’s effort to position ahandheld cardiac ultrasound to displace the stethoscope, rather than to disrupt the expensive fixed ultrasound machine.
H/T Healthcaresavvy.wbur.org
Saturday, March 24, 2012
We’re Number One
 |
| Click on image to enlarge. Source |
The Blue Cross Blue Shield of Massachusetts Foundation just published a great 50-slide deck of graphics comparing health care cost and utilization in Massachusetts with the rest of the country. Massachusetts has the highest cost of health care in the country, and the largest number of physicians per capita. Our physicians are more likely to be specialists than in the rest of the country. Our hospitals are more than twice as likely to be academic medical centers. Our health insurance designs are among the richest around, with low average deductibles.
Most of the increased cost of care since Massachusetts’s health care reform has been cost per unit, not increased utilization. The rate of cost increase in Massachusetts has been lower than the rest of the country since we passed our health care reform, although of course we started at a much higher base.
Implications of Massachusetts experience for the post-ACA American health care system:
· Increasing access doesn’t lead to an instant onslaught of new utilization
· Health care is regional –and structural issues (not health care reform) make health care in Massachusetts spectacularly expensive
· We need to keep our eyes on price – not just utilization – if we want to control the rate of health care inflation
* Health care inflation crowds out other important societal priorities (see graphic at the bottom of this post. That's why health care reform, and control of health care costs are so important.
The Blue Cross Blue Shield Foundation conclusions:
- Massachusetts spends more on health care than any other state.
- Higher costs were not caused or markedly accelerated by health reform, as Massachusetts has been a high spending state for years.
- The underlying difference in spending between Massachusetts and the U.S. overall is rooted in the state’s demographics, insurance coverage, and health care market structure, which includes disproportionately many specialists and teaching hospitals and some very large and powerful hospital systems.
- Though the amount of most services used increases every year, the majority of the growth in health spending comes from increased prices.
- There is enormous variation in total health care spending across the state, stemming from variations in both price and utilization.
- However, neither higher prices nor higher utilization of services is associated with higher quality or better health outcomes, suggesting that there is a significant amount of waste in the Massachusetts health care system. It also suggests that costs can be lowered without decreasing overall quality or health outcomes.
 |
| Click image to enlarge. Source |
Wednesday, March 21, 2012
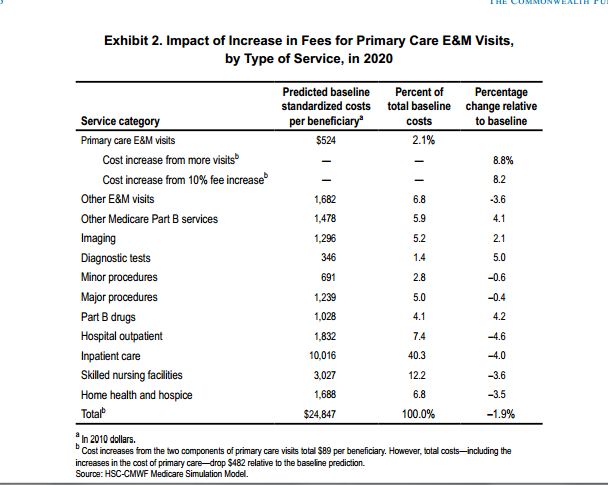
Commonwealth Fund Sees Medicare Savings From PCP Fee Increases
Today’s Managing Health Care Costs Indicator is 2%
The Commonwealth Fund projects that Medicare investing through maintaining the Affordable Care Act’s 10% primary care physician increase beyond expiration in 2016, Medicare could save almost two percent of total costs. In this simulation, primary care costs would go up by $89 per person per year (about equally distributed between increased unit costs and increased utilization), while total costs would decrease by $539 – a whopping 6:1 return on investment.
The authors posit that savings would come from hospitals and outpatient hospital facility fees and specialist care. Imaging and diagnostic costs increase in this simulation, which seems unlikely, as specialists seem as happy to order tests as primary care physicians. Outpatient medications and other Part B services also increase.
The authors make a powerful case to make more investments in primary care. The savings could presumably increase further if the primary method of payment was not fee for service.
 |
| Click on image to enlarge. Source link above |
CBO Weighs In: Insurance Costs Up and Coverage Down Without Individual Mandate
Today’s Managing Health Care Costs Indicator is 16 milllion
The CBO estimates that 16 million fewer people would have health care coverage in 2021 if the individual mandate is eliminated . The deficit would be $282 billion lower over the decade (the net of $149 billion less Medicaid spending, business and exchange subsidies, loss of penalties, and higher tax revenue as there are fewer claiming health care deductions.
However, the cost of purchasing insurance in the nongroup pool would go up a whopping 15-20% - largely because those likely to opt out of health insurance are likely to be the healthiest.
Two observations. Some have suggested that the cost of health care reform has gone up substantially (as much as doubled) since the last estimates. Ezra KIein shows that this is false - the only increased cost is higher subsidies due to just how bad the Great Recession has been. Beware comparisons of different years, especially when the earlier estimate included pre-implementation years!
The second observation is that government expenditures of $282 billion to have 16 million additional insured Americans at the end of 10 years is a good deal. (I’d like to calculate how much this is per person insured per year, but I can’t find the year-by-year information among the CBO publications.) Some of those who will be insured under the mandate but would go “naked” absent the penalty will be healthy. But remember that health insurance is wealth transfer from the healthy to those with illnesses – so we NEED to get healthy people to participate in health insurance. Health insurance cannot be affordable if only the sick participate.
The mandate is associated with very low opt-out rates in Massachusetts, despite a very small penalty. Supreme Court has oral arguments in just a few days.
Tuesday, March 20, 2012
New England Journal at 200, and Disruptive vs. Accretive Innovation
Today’s Managing Health Care Costs Indicator is 200
From the Times:
In [Relman’s] ideal health care system, doctors would be salaried and organized into large multispecialty group practices similar to the Mayo Clinic and other private clinics; care would be delivered by a single-payer nonprofit system, financed by the taxpayers. “You’d save an enormous amount of money,” he said, much of it by eliminating the private insurance industry, “a parasite on the health care system.”
There is more nuance to the role of profit in health care than Relman and Angell would allow. The pharmaceutical industry might have many profiteers – and the return on capital for the pharmas has historically been high. Further, it often seems that the pharmaceutical industry spends more energy on marketing “me too” drugs and promoting new medications that are much more expensive but only a tiny bit more effective than existing generics. BUT – and it’s a big but – most of the major improvements in medical care in my professional lifetime have come from pharmas. This includes highly active antiretroviral therapy (HAART) for HIV, gleevec for chronic myelocytic leukemia, and drugs that aim at specific genetic targets for breast and lung cancer. For-profit companies have led the way in accretive innovation – the innovation that layers on new technology or new approaches to increase quality (often just a little), and also to increase revenue and cost (often a lot).
Can for-profit companies play a meaningful role in disruptive innovation, where there are large increases in value – often associated with small initial sacrifices in quality? I’d suggest the answer is unequivocally “yes,” as long as the market will reward disruptive innovation. Toshiba (a for-profit company) created the MRI machine that profitably performs $100 MRI scans for the Japanese market where price regulation didn’t allow for $1000 scans. General Electric has developed in its labs (in India) inexpensive PC-based EKG machines and a low-cost hand-held cardiac ultrasound. Ironically, of course, in the US GE would like to position the handheld cardiac ultrasound to replace the stethoscope (thus increasing cost) rather than the fixed ultrasound. In the US, where higher payment is possible for improvements in quality that often have little or no clinical value, even potentially disruptive innovation is transformed into accretive innovation. See this post for more ruminations on this example.
I’m not convinced that the profit status of a company alone determines how effective it will be at delivering value in health care. There are plenty of high-priced not-for-profit hospital systems and there are plenty of high value physician-owned offices. I do think that how the company is paid – including the price-sensitivity of purchasers and public knowledge of quality – plays a substantial role in determining whether companies increase value, or merely increase revenue. I think we need to focus on effective payment reform to increase value in health care, and then encourage competition of both for-profits and not-for-profits.
I blogged about Arnold Relman’s complaints about the Affordable Care Act last fall.
There’s more about the NEJM’s 200th anniversary. For the skeptical, check out On the Media’s interview with Jeffrey Drazen, the current editor, who talks about the many nostrums that were at one time promoted in its pages. The Journal at one point supported eugenics, pathologized homosexuality, and editorialized against women in medicine. It was published for almost a half century before the germ theory of disease became popular. Drazen notes
The key thing is to recognize you made a mistake and try to make progress.
The New England Journal has also been a market leader in making its articles available for no cost to those logging in from developing countries, and making articles with important clinical or public policy implications free immediately to all. Happy Birthday.
Monday, March 19, 2012
CDC Chief and Graphic Antismoking Ads
Today’s Managing Health Care Costs Indicator is $200 billion
Thomas Frieden, the Director of the Centers for Disease Control and Prevention (CDC) is interviewed in this weekend’s On The Media, where he talks about the federal government’s upcoming graphic anticigarette ad campaign. He quotes freely from the most recent Surgeon General’s Report on Smoking, which focuses on preventing smoking among youth.
Smoking continues to be the leading cause of preventable death in the US – almost a half-century after the first Surgeon General’s report. Still – the rate of adult cigarette smoking in the US has plummeted by half, and the huge drop in death from heart disease is likely largely due to smoking cessation (rather than cholesterol medications or heart surgery or angioplasty).
A few facts mentioned by Dr. Frieden:
- For each person who dies of a smoking-related disease, 20 are disabled or made ill from smoking
- The annual cost of smoking to the national economy is estimated to be $200 billion. (This is loss of productivity – not only health care claims costs)
- 2/3 of smokers want to quit
- Most people who ever smoked have already quit
- Most smokers try to quit each year.
He hopes the ad campaign will help convince 50,000 smokers to quit.
Here’s what this campaign is up against (From the 2012 Surgeon General’s Report, p10)
In 2008, tobacco companies spent $9.94 billion on the marketing of cigarettes and $547 million on the marketing of smokeless tobacco. Spending on cigarette marketing is 48% higher than in 1998, the year of the Master Settlement Agreement. Expenditures for marketing smokeless tobacco are 277% higher than in 1998.
Subscribe to:
Posts (Atom)